
When Your Disease Has a "Bad" Name, Should Patients & Caregivers Be Part of the Discourse?
A 40 year debate around the name of my disease may come to an end soon.

Hello Beautiful Readers,
I’ll start saying, candidly, this post may seem like “inside baseball” to my non-aHUS family but it’s a huge headline for me.
If you get to the bottom of the post, I’ll reward you with a cute photo of July.
I was diagnosed with aHUS as you all know. But I may not have aHUS anymore, and not because I’m cured. There’s a big movement to change the disease name.
Recently an article was released by a team of medical clinician experts in TMA or thrombotic microangiopathy (which means tiny blood clots) suggesting a change to the name of my disease aHUS or atypical Hemolytic Uremic Syndrome.
For context, TMA or tiny blood clots erupted in my body after I gave birth causing multiple organ failure.
Changing the name of a disease is not a simple matter, and a central question exists - should patients and caregivers be part of the process?
In the end, I want a name that saves lives but rebranding a disease will take a great deal of heavy lifting and finding consensus.
Team aHUS or Team TMA?
I wrote recently about the history of my disease aHUS - so you can bring yourself up to speed on that if you missed it.
About 40 years ago, discussion emerged about how atypical HUS was a broadly ineffective name. Folks in the medical community suggested a change saying the name only tells us what the disease IS NOT - instead of what it in fact IS.
Essentially, it’s a broad, bad name.
Now clinician authors of the article urge that the challenge in the name aHUS leads to a challenge in diagnosis.
First, I can see what a pickle debating all this must have been. It sounds like everyone agrees on the need for change, so I can get behind that.
But I have questions.
Their suggestions for what they think we should call this disease - or series of diseases - is essentially a prefix stating the cause of the disease or if there’s a known TMA type and then the term “TMA.”
Here’s where we get more complicated.
SO, TMA is the foundational name of the disease - which I’m all for actually. But the prefix creates a lot of buckets, and a super long photo caption below.
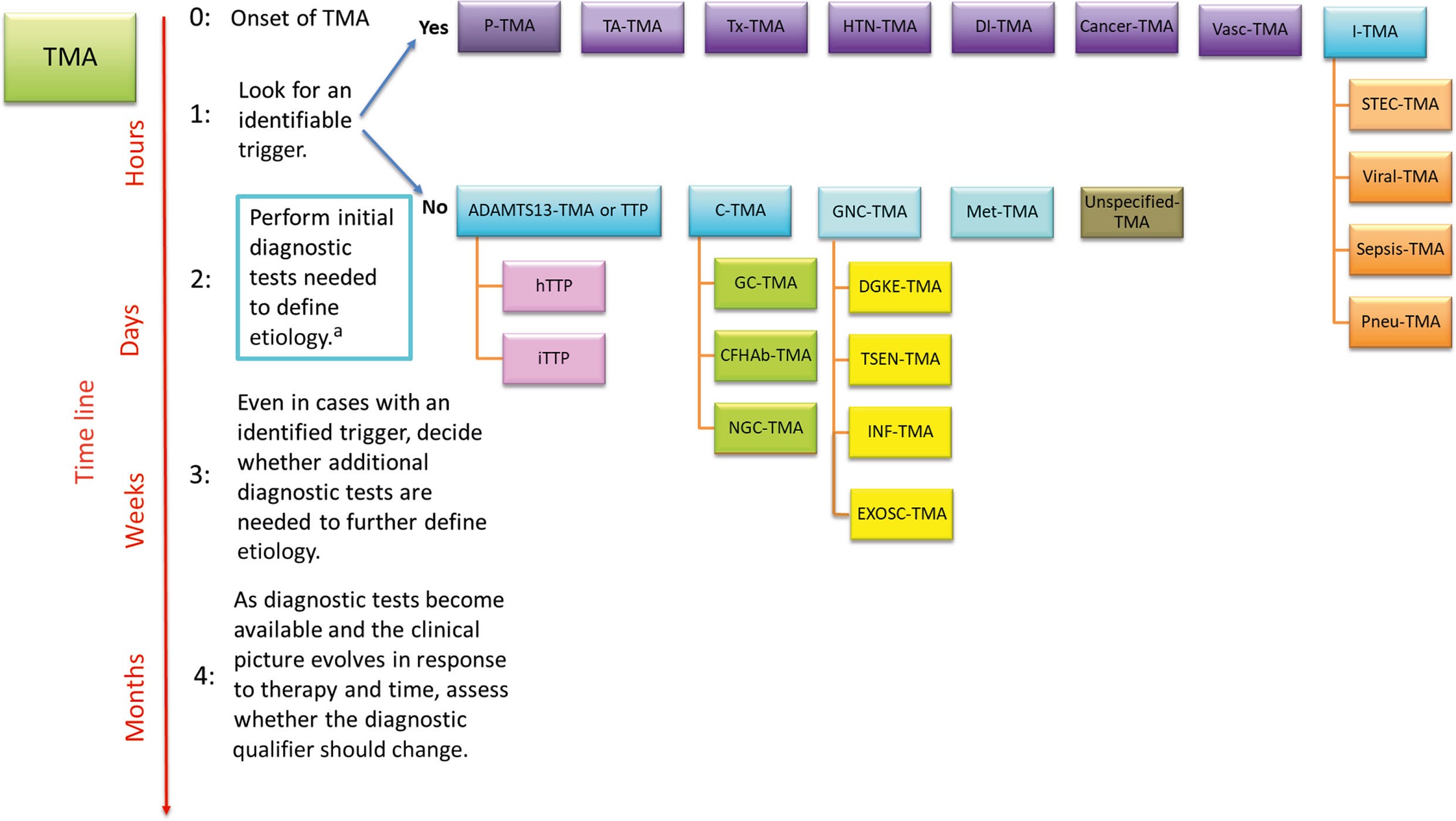
The prefix, according to the article, would essentially be fluid as physicians solve more mysteries about the trigger and the specific TMA details.
Did I lose you? Because this prefix part does feel a bit overwhelming and frankly I’m less a fan of “fluid prefixes.”
If calling something TMA helps diagnose the disease - great. Let’s do it.
For me - and let’s be honest, no one asked patients what they think - I like just TMA. The prefix buckets lose me. In rare disease, it just makes me feel EVEN MORE RARE. Sure, maybe clinically it’s helpful for a doctor, but for me it’s a lot of alphabet soup.
Plus we may share various triggers or paths to the TMA, but patients and caregivers are certainly bonded by the aggressive ravage TMA causes. We share that in common distinctively.
Now I’m gonna get extra inside baseball so feel free to skip this paragraph if you’re not TMA-curious; read this article for background on the disease itself if you want to follow this thought-thread. The complement-mediated part feels murky because some of us don’t test positive for a gene, but that doesn’t mean we don’t have a mutated gene. It could mean it’s just not been discovered yet? But we do respond to the complement inhibitor drug - so wouldn’t that mean it’s by nature a complement over-activation regardless of a found mutated gene? Physicians feel free to respond because this one of outside my Theatre BA.
Anyways beyond physician debates, patients and caregivers aren’t huge fans of change. We are attached to our patient groups. We bought the aHUS water bottle. Some started entire advocacy organizations with urls, brands, names and have worked tirelessly for aHUS awareness. There’s even a DAY, September 24th! Mark your calendar!
But we are also pro-Science and we want what’s best for us all, clinicians and patients alike, at the end of the day.
And then we need make sure insurance companies know about it because I could see this being a pain in the butt come pricey complement inhibitor drug pre-approval time. Is there a plan? Is there a central organization who helps spread the word? Is there a project manager on this rebrand?
It’s an exhausting pivot. But I do believe if there is a campaign to explain the “why” in a cogent manner, the community will support it. But it needs stakeholder aHUS advocacy buy-in - and I’m not sure I’m seeing that play-out from the sidelines.
For what it’s worth, I do think patients and caregivers should be consulted. The name of the disease affects us greatly.
My dear friend with metastatic breast cancer informed me the other day it’s not causally called “metastatic breast cancer” - there’s an element of thoughtful branding involved. No one wants Stage 4 Cancer. No one wants to say they live at Stage 4. So, they have a name that considers the patient’s well-being and mental health. It’s a patient’s first name.
None of the convo around my disease feels candidly very “patients-first,” except for the more direct path to new patient diagnosis.
We have to live with a name that washes over people like a list of salad dressings shared too fast by a triple-sat waiter phoning it in during dinner rush.
No one hears it and everyone just goes “whoa that sounds bad.” In one ear and out the other.
As the BBC article suggests, I’m not sure this a great solution either: “WHO recommended in May 2015 that new human diseases be given socially acceptable names. These are names that include "generic descriptive terms" based on things such as symptoms and severity rather using the names of person or a specific location. But some new names might be too complex or easy to grasp.”
"A lot of the diseases I treat are such complicated diseases - you would need 10 words to describe them," explained Dr Hughes, the rheumatologist named for Hughes Disease.
And that’s where we find ourselves: multi-name, too many acronyms land.
But, again, no one asked me what I thought of a name… or any of us. But I do wonder what it would look like for the disease community itself to weigh in?
We might end up with something like Chronic Micro-Blood Clot Disorder. But would that be so bad?
Apologies to all the cringing TMA physicians. Thank you for your service! I am grateful.
For more, I encourage you to read Len’s article at the aHUS Alliance page.
Patients/Caregivers, what do you think of a name change? Can you get behind it?

Here’s a reward photo of July and a tiny pumpkin.
More on aHUS or CM-TMA or P-TMA or Whatever it’s Called:
aHUS Q&A

A medical student reached out to me with questions about atypical HUS, so I made the video response below.

Welcome to my disease. What is atypical Hemolytic Uremic Syndrome (aHUS) or Complement-Mediated Thrombotic Microangiopathy (CM-TMA)?

Hi, If you’re new here, I started writing a book six months ago when I was on dialysis. It’s intended to be both memoir and a practical tool to help folks who might be going through something similar or those caregivers and family supporting someone with a challenging diagnosis. I hope to include excerpts here as I write. NOTE: This is not intended to r…
I started writing this when I was on dialysis. It’s intended to be both memoir and a practical tool to help folks who might be going through something similar or those caregivers and family supporting someone with a challenging diagnosis. NOTE: This is not intended to replace actual medical guidance. Please consult your doctors on your individual challenges and situations. Please talk to your clinicians before adjusting any of your care protocols. Also names have been changed for most of my medical staff.
Thank you to CC Couchois, Roy Lenn, and Dr. Richard Burwick for your founding level donation.
Taylor you are absolutely right, I agree with everything you are saying! While I do like the term aHUS, I am also part of the group that agreed to update the terminology. TMA is a useful umbrella term but the question remains, which of the TMA’s are aHUS and require complement blockade? For example, I’m interested in pregnancy TMA which includes HELLP syndrome, TTP, and aHUS. Both HELLP and aHUS may be considered complement mediated TMA, but how do we prove complement is the problem? Truthfully, we are still left in a conundrum, but I hope that ultimately the TMA terminology will bring our communities together, and bring more attention to aHUS and other rare TMA disorders. Thank you for all that you do for the aHUS/TMA community!